Hip Ultrasound: Advantages and limitations
Overview
Hip pain is a common complaint with many causes. The two most common causes of pain around the hip are the hip joint itself (most commonly wear and tear), and inflammation of the greater trochanteric bursa at the side of the hip. The hip joint is deeply located in the groin area. Only the surface of the joint can be seen on ultrasound. Although this can show potential issues with the joint, such as wear and tear and inflammation, the deeper portion of the joint and the inner cartilage lining are not readily amenable to ultrasound assessment. The surrounding soft tissue structures are however excellently seen on ultrasound. This includes the joint capsule, tendons ligaments and bursae. Ultrasound is also the first-line assessment for other causes of groin pain, such as hernias.
Common painful conditions around the hip
Greater trochanteric pain syndrome
Greater trochanteric pain syndrome is a condition characterised by pain and tenderness around the side of the hip. The symptoms often start as a light pain, exacerbated on walking, or when lying on the side. It can progress to severe debilitating pain. The pain can radiate to the buttock area or along the side of the thigh.
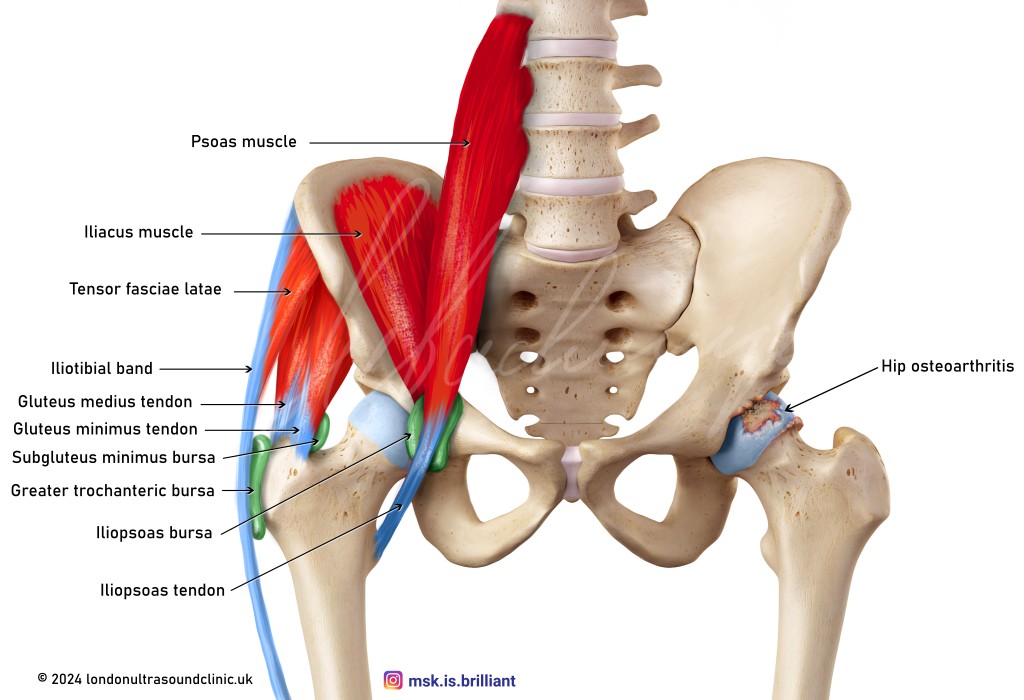
Important muscles and tendons are attached to the outer bony prominence of the hip (the greater trochanter). These muscles and tendons play a crucial role in the walking cycle. The iliotibial band is a strong tendinous structure that comes from the pelvis and extends along the outer aspect of the hip and down to the knee. At the point where it passes over the greater trochanter, it is prone to friction, overuse, and inflammation. The greater trochanteric bursa, located between the bone and the band, serves as a cushion to reduce friction (see Figure 1). It can itself become inflamed and painful.
All of those structures can be involved in greater trochanteric pain syndrome, namely the:
- Gluteal medius and gluteus minminus tendons, the
- Greater trochanteric bursa, and the
- Iliotibial band.
Those structures are located closely together, and a combination of those structures is often responsible for the pain [1].
Greater trochanteric bursitis
Greater trochanteric bursitis is an inflammation of the bursa at the side of the hip. It is usually caused by overuse, prolonged pressure to the area, or by abnormal biomechanics of the gait. It can also be caused by acute traumatic events. Bone spurs along the bony surface of the greater trochanter can further contribute to irritation of the bursa.
Ultrasound can show thickening or fluid distension of the bursa. In mild forms of bursitis, the ultrasound appearances may be normal, but it may still help to confirm the source of the pain by identifying the maximum point of tenderness. There are further smaller bursae around the outer hip, which can get inflamed and painful, namely the subbgluteus medius bursa and the subbgluteus minimus bursa. They are located deep to their corresponding tendons.
Gluteus medius and gluteus minimus tendinosis
The gluteus medius and minimus muscles are located at the side of the hip, and their tendons attach at the tip of the greater trochanter, which is the prominent bone at the side of the hip. They play a crucial role in maintaining the tilt of the pelvis during the walking cycle. As a result of overuse, injury, or abnormal hip biomechanics they can get thickened and inflamed, called gluteal tendinopathy. This can progress to tears. The symptoms are that of greater trochanteric pain syndrome.
An ultrasound scan can demonstrate the tendon abnormality. A tendinopathic tendon appears thickening, and it loses the typical bright and fibrillar appearance of a normal tendon. Tears of the tendon can also be demonstrated [2].
Osteoarthritis
Osteoarthritis refers to ‘wear and tear’ of the joint. Both sides of the hip joint, the socked and the ball, are covered by a cartilage lining, ensuring smooth gliding during motion of the joint. In Osteoarthritis this cartilage lining gradually degenerates and becomes thinner, till the bones of the socket and the cup get into direct contact. The joint compensates by forming bone spurs around the joint.
Traditionally, radiographs (X-rays) are used to diagnose and monitor the progress of hip osteoarthritis. More recently, the potential value of ultrasound in evaluating hip osteoarthritis has been described [3], [4]. Ultrasound can demonstrate the bone spur formation at the front of the joint, and potentially lesions in the cartilage lining. Besides this, it can show secondary changes such as thickening and inflammation of the joint capsule and excessive fluid accumulation inside the joint. The fluid accumulation (joint effusion) is a reaction of the joint to irritation or inflammation. These findings are invisible on X-rays and would otherwise require an MRI scan to show. Despite this X-ray remains the first-line test for hip osteoarthritis.
Iliopsoas tendon
The iliopsoas tendon is located at the front of the hip joint. It helps to bend the hip joint forward and is therefore another crucial tendon involved in the walking cycle. Abnormalities around the iliopsoas tendon, albeit rare, can cause hip pain. The pain is often felt deep in the groin and exacerbated by actions requiring the iliopsoas tendon, such as raising the knee.
Iliopsoas bursitis
The psoas tendon comes from the spine and passes through the pelvis and along the front of the hip joint. Here, it is surrounded by a bursa to improve the gliding of the tendon against the hip and the pelvis during movements. With overuse, the burse can get irritated and inflamed, forming too much fluid and resulting in bursitis.
Snapping hip syndrome: Snapping iliopsoas tendon
Snapping hip syndrome is a palpable or audible snap around the groin, that occurs on certain hip movements. Whilst the snapping can have multiple causes (including from inside the hip joint and from structures around the joint), the snapping iliopsoas tendon is one of the causes that can be demonstrated on ultrasound [5].
Inguinal hernia
Inguinal hernias are a common culprit in patients with hip and groin pain. Inguinal hernias occur when fatty tissue or even part of the bowel protrudes through a weak point in the abdominal wall. This can happen directly through a small defect in the wall or indirectly through a pre-existing canal called the inguinal canal. Sometimes, hernias create noticeable lumps in the groin area and cause discomfort, but they can also be present without causing any pain. Surprisingly, even small hernias can be a source of pain.
Ultrasound is the go-to tool when it comes to examining lumps in the groin and diagnosing hernias[6]. Ultrasound allows to capture of dynamic views of the hernia. In other words, we can see how the hernia behaves, as it may come and go depending on your activities or movements. During the ultrasound examination, the size of the hernia and its relation to the surrounding structures can be assessed, which will help the surgeons plan the treatment.
Ultrasound-guided procedures around the hip
Ultrasound is excellent for imaged-guided procedures, such as steroid injections into the joint (for osteoarthritis), to the greater trochanteric bursa (for bursitis or gluteal tendonitis), and around the iliopsoas tendon (for iliopsoas bursitis or tendonitis).

Dr M Siebachmeyer
Musculoskeletal radiologist based at St Georges Hospital, London.
References
[1] S. S. Long, D. E. Surrey, and L. N. Nazarian, “Sonography of greater trochanteric pain syndrome and the rarity of primary bursitis,” AJR Am J Roentgenol, vol. 201, no. 5, pp. 1083–1086, Nov. 2013, doi: 10.2214/AJR.12.10038.
[2] S. I. Docking et al., “Identification and differentiation of gluteus medius tendon pathology using ultrasound and magnetic resonance imaging,” Musculoskelet Sci Pract, vol. 41, pp. 1–5, Jun. 2019, doi: 10.1016/J.MSKSP.2019.01.011.
[3] S. N. Sudula, “Imaging the hip joint in osteoarthritis: A place for ultrasound?,” Ultrasound: Journal of the British Medical Ultrasound Society, vol. 24, no. 2, p. 111, 2016, doi: 10.1177/1742271X16643118.
[4] S. Clausen, S. Kjær, U. Fredberg, L. Terslev, J. Hartvigsen, and B. Arnbak, “Ultrasound imaging in patients with hip pain and suspected hip osteoarthritis: an inter-rater and intra-rater reliability study,” BMJ Open, vol. 10, no. 11, Nov. 2020, doi: 10.1136/BMJOPEN-2020-038643.
[5] M. Piechota, J. Maczuch, J. Skupiński, K. Kukawska-Sysio, and W. Wawrzynek, “Internal snapping hip syndrome in dynamic ultrasonography,” J Ultrason, vol. 16, no. 66, p. 296, Sep. 2016, doi: 10.15557/JOU.2016.0030.
[6] W.-T. Wu, K.-V. Chang, C.-P. Lin, C.-C. Yeh, and L. Ozcakar, “Ultrasound imaging for inguinal hernia: a pictorial review,” Ultrasonography, vol. 41, no. 3, Jul. 2022, doi: 10.14366/USG.21192.