Hand and Wrist Ultrasound
The recent advances in ultrasound technology allow it to provide excellent information regarding the soft tissues of the hand and wrist. Ultrasound is considered the first-line test for tendon and ligament injury, inflammatory arthritis, tendinitis, tenosynovitis, and lumps and bumps around the wrist and hand. It is also used to guide steroid injections and in the treatment of ganglion cysts and many other conditions.
Rheumatoid arthritis (RA) and psoriatic arthritis (PA)
Rheumatoid and psoriatic arthritis are the most common inflammatory joint problems in the hand. They can lead to significant disability if not detected and treated early. In the past, rheumatoid arthritis was evaluated only with radiographs. However by the time erosions become visible on X-rays, the joint has already undergone significant destruction. Today, the aim is to diagnose and treat rheumatoid arthritis before it causes structural damage to the joints, therefore minimising the risk of long-term disability.
The European Alliance of Associations for Rheumatology (EULAR) now recommends ultrasound as the first-line test in patients with suspected RA[1]. It recommends that patients are scanned by a trained clinician using a standardised approach to ensure all relevant structures are assessed. This includes the tendons, joints, and the carpal tunnel.
Tendon inflammation is easily visible on ultrasound. Actively inflamed joints have effusions (accumulation of joint water) and inflammation in the synovium, the inner joint lining. This can be seen as synovial thickening with increased blood flow, i.e. Doppler activity (Figure 1). Ultrasound can even detect erosions (Figure 2).


The severity of inflammation determines the treatment for rheumatoid arthritis and psoriatic arthritis. Ultrasound severity is scored on a scale of 0 to 3[2]. Grading assists the rheumatologist in selecting the most appropriate treatment and monitoring the response to treatment during follow-up ultrasound examinations.
Gout and CPPD
Gout and pseudogout, also known as calcium pyrophosphate deposition disease (CPPD), occur when crystals accumulate in the joints. They are usually diagnosed by clinical manifestations, blood tests, and radiographs. However, in challenging cases, ultrasound can be useful. In gout, the high-density soft tissue thickening around joints (gout tophi) can be readily seen. Within the joints, the gout crystal can be seen covering the surface of the joint cartilage, creating a typical double contour sign. In contrast, CPPD crystals tend to occur more centrally in the cartilage. These two distinct features can help to distinguish gout from pseudogout on ultrasound.
Tendinitis and tenosynovitis
Tendinitis and tenosynovitis (inflammation of the tendon or the surrounding tendon sheath) often accompany rheumatoid arthritis. But they also occur because of overuse.
A classic example of overuse is De Quervain’s tenosynovitis which causes pain around the wrist and forearm. Repetitive movements such as lifting a child can aggravate it (Figure 3).

Rheumatoid arthritis usually affects the extensor carpi ulnaris tendon located on the outer wrist. Furthermore, the flexor tendon that runs down the front side of the forearm can also become inflamed, resulting in pain and stiffness in the fingers.
Trigger finger
Trigger finger, also known as stenosing tenosynovitis, causes stiffness and locking of the finger when the finger is bent or straightened. This is caused by the thickening and tightening of the tendon sheath, which acts as a tunnel for the tendon and stabilises its course. It can also be caused by swelling of the tendon.
On ultrasound, both the tendon and tendon sheath can be assessed, and it is possible to see the thickening that causes the ‘catching’ of the tendon in the tunnel (Figure 4). Ultrasound allows dynamic evaluation of the tendon while the patient moves the finger, directly demonstrating the triggering (Figure 5).

Ultrasound is used to guide steroid injection into the tendon sheath. This can help reduce swelling and stiffness and improve the symptoms of the trigger finger. Additionally, during the procedure, the thickened portion of the tunnel can be released using a needle after numbing the area with local anaesthetics [3]. This procedure is called percutaneous trigger finger release and is usually only performed after assessment by a specialist.
Ganglion cysts and other lumps and bumps
Lumps and bumps around the wrist are common complaints. They are most commonly caused by a ganglion cyst. They can occur around joints or along the course of tendons and they consist of a thick, jelly-like fluid. There are however many other types of lesions, that present as a lump, most of which are benign, but rarely they can also be tumours. Ultrasound is used to define the nature of the lesion and to rule out any serious issues.
Once ultrasound confirms a ganglion cyst, it can help drain the cyst using a needle. Ultrasound helps to direct the needle in the correct place and avoid damage to neighbouring blood vessels and nerves. Ultrasound guidance is particularly useful when treating cysts located deep below the skin.
Other common lumps around the wrist and hand are Dupuytren contracture (Figure 6), nodules related to the tendons, such as giant cell tumours, lipomas, and epidermal inclusion cysts.

Carpal tunnel syndrome / Median nerve impingement
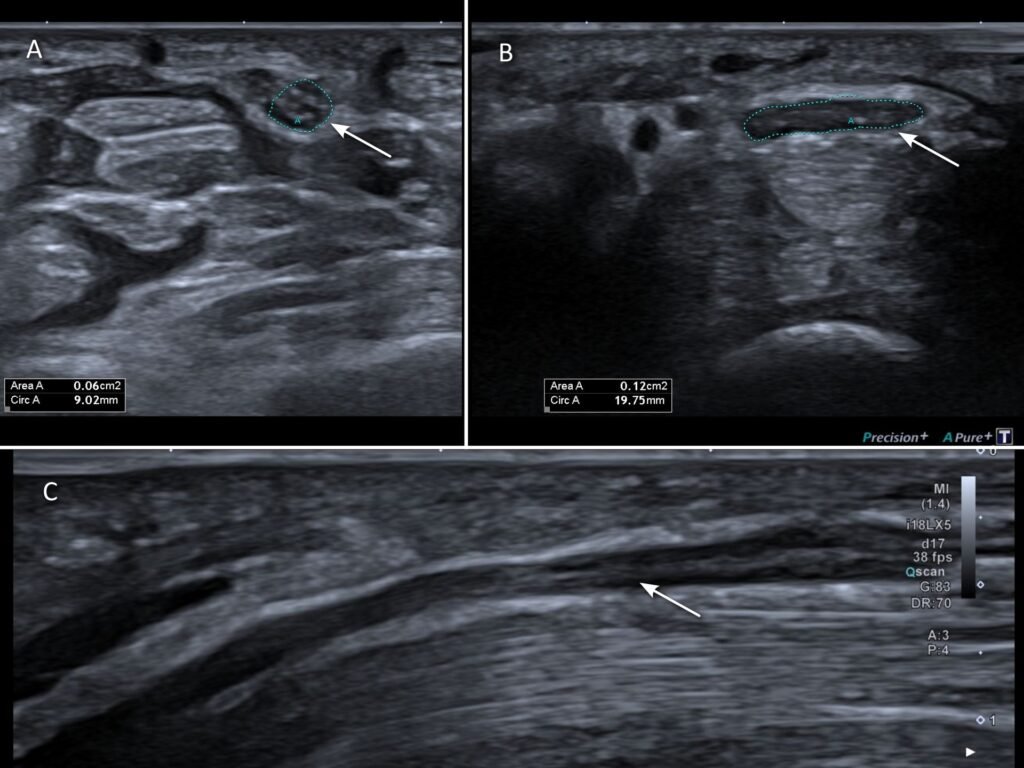
Carpal tunnel syndrome is one of the most common nerve entrapment syndromes. When the median nerve (the main nerve running down the front of the forearm) gets irritated passing through the tight carpal tunnel, it can cause sensory and motor dysfunction around the thumb and index finger.
Clinical evaluation and nerve conduction testing are often performed to confirm the diagnosis.
Changes of the median nerve seen on ultrasound very accurately predict carpal tunnel syndrome. Multiple parameters are considered when evaluating for carpal tunnel syndrome, such as thickening and flattening of the nerve [4] (Figure 7), as well as swelling of the overall carpal tunnel content.
Steroid injections are often used to reduce swelling and nerve irritation before proceeding to surgery. This will be done with ultrasound to ensure accurate needle positioning during the injection.

Dr M Siebachmeyer
Musculoskeletal radiologist based at St Georges Hospital, London.
Reference
[1] A. N. Colebatch et al., “EULAR recommendations for the use of imaging of the joints in the clinical management of rheumatoid arthritis,” Ann Rheum Dis, vol. 72, no. 6, pp. 804–814, Jun. 2013, doi: 10.1136/ANNRHEUMDIS-2012-203158.
[2] M. A. D’Agostino et al., “Scoring ultrasound synovitis in rheumatoid arthritis: a EULAR-OMERACT ultrasound taskforce – Part 1: definition and development of a standardised, consensus-based scoring system,” RMD Open, vol. 3, no. 1, Jul. 2017, doi: 10.1136/RMDOPEN-2016-000428.
[3] F. Lapegue et al., “Us-guided Percutaneous release of the trigger finger by using a 21-gauge needle: A prospective study of 60 cases1,” Radiology, vol. 280, no. 2, pp. 493–499, Aug. 2016, doi: 10.1148/RADIOL.2016151886/ASSET/IMAGES/LARGE/RADIOL.2016151886.TBL1.JPEG.
[4] B. Elnady et al., “Diagnostic potential of ultrasound in carpal tunnel syndrome with different etiologies: Correlation of sonographic median nerve measures with electrodiagnostic severity,” BMC Musculoskelet Disord, vol. 20, no. 1, pp. 1–8, Dec. 2019, doi: 10.1186/S12891-019-3010-5/TABLES/4.